How to resolve AdBlock issue?
How to resolve AdBlock issue? 
News

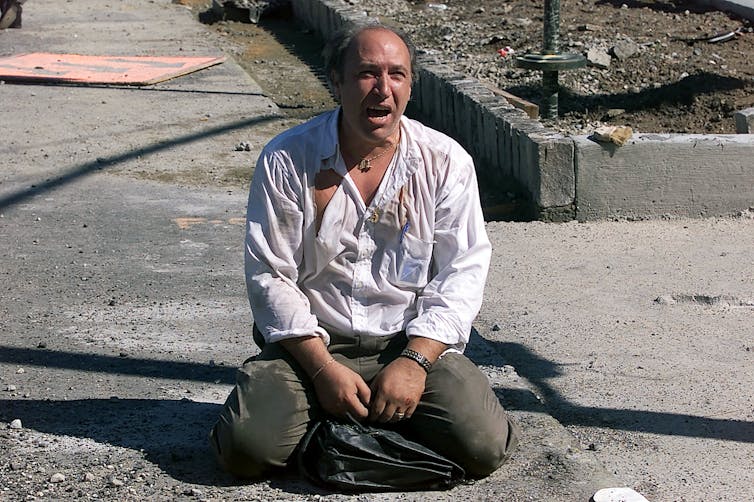
The 9/11 terrorist attack on the World Trade Center in New York resulted in the loss of 2,753 people in the Twin Towers and surrounding area. After the attack, more than 100,000 responders and recovery workers from every U.S. state – along with some 400,000 residents and other workers around ground zero – were exposed to a toxic cloud of dust that fell as a ghostly, thick layer of ash and then hung in the air for more than three months.
The World Trade Center dust plume, or WTC dust, consisted of a dangerous mixture of cement dust and particles, asbestos and a class of chemicals called persistent organic pollutants. These include cancer-causing dioxins and polyaromatic hydrocarbons, or PAHs, which are byproducts of fuel combustion.
The dust also contained heavy metals that are known to be poisonous to the human body and brain, such as lead – used in the manufacturing of flexible electrical cables – and mercury, which is found in float valves, switches and fluorescent lamps. The dust also contained cadmium, a carcinogen toxic to the kidneys that is used in the manufacturing of electric batteries and pigments for paints.

Polychlorinated biphenyls, human-made chemicals used in electrical transformers, were also part of the toxic stew. PCBs are known to be carcinogenic, toxic to the nervous system and disruptive to the reproductive system. But they became even more harmful when incinerated at high heat from the jets’ fuel combustion and then carried by very fine particles.
WTC dust was made up of both “large” particulate matter and very small, fine and ultrafine ones. These particularly small particles are known to be highly toxic, especially to the nervous system since they can travel directly through the nasal cavity to the brain.
Many first responders and others who were directly exposed to the dust developed a severe and persistent cough that lasted for a month, on average. They were treated at Mount Sinai Hospital and received care at the Clinic of Occupational Medicine, a well-known center for work-related diseases.
I am a physician specializing in occupational medicine who began working directly with 9/11 survivors in my role as director of the WTC Health Program Data Center at Mount Sinai beginning in 2012. That program collects data, as well as monitors and oversees the public health of WTC rescue and recovery workers. After eight years in that role, I moved to Florida International University in Miami, where I am planning to continue working with 9/11 responders who are moving to Florida as they reach retirement age.

From acute to chronic conditions
After the initial “acute” health problems that 9/11 responders faced, they soon began experiencing a wave of chronic diseases that continue to affect them 20 years later. The persistent cough gave way to respiratory diseases such as asthma, chronic obstructive pulmonary disease (COPD) and upper airway diseases such as chronic rhinosinusitis, laryngitis and nasopharyngitis.
The litany of respiratory diseases also put many of them at risk for gastroesophageal reflux disease (GERD), which occurs at a higher rate in WTC survivors than in the general population. This condition occurs when stomach acids reenter the esophagus, or food pipe, that connects the stomach to the throat. As a consequence of either the airway or the digestive disorders, many of these survivors also struggle with sleep apnea, which requires additional treatments.
Further compounding the tragedy, about eight years after the attacks, cancers began to turn up in 9/11 survivors. These include tumors of the blood and lymphoid tissues such as lymphoma, myeloma and leukemia, which are well known to affect workers exposed to carcinogens in the workplace. But survivors also suffer from other cancers, including breast, head and neck, prostate, lung and thyroid cancers.
Some have also developed mesothelioma, an aggressive form of cancer related to exposure to asbestos. Asbestos was used in the early construction of the north tower until public advocacy and broader awareness of its health dangers brought its use to a halt.
And the psychological trauma that 9/11 survivors experienced has left many suffering from persistent mental health challenges. One study published in 2020 found that of more than 16,000 WTC responders for whom data was collected, nearly half reported a need for mental health care, and 20% of those who were directly affected developed post-traumatic stress disorder.
Many have told me that the contact they had with parts of human bodies or with the deadly scene and the tragic days afterward left a permanent mark on their lives. They are unable to forget the images, and many of them suffer from mood disorders as well as cognitive impairments and other behavioral issues, including substance use disorder.
An aging generation of survivors
Now, 20 years on, these survivors face a new challenge as they age and move toward retirement – a difficult life transition that can sometimes lead to mental health decline. Prior to retirement, the daily drumbeat of work activity and a steady schedule often helps keep the mind busy. But retirement can sometimes leave a void – one that for 9/11 survivors is too often filled with unwanted memories of the noises, smells, fear and despair of that terrible day and the days that followed. Many survivors have told me they do not want to return to Manhattan and certainly not to the WTC.
Aging can also bring with it forgetfulness and other cognitive challenges. But studies show that these natural processes are accelerated and more severe in 9/11 survivors, similar to the experience of veterans from war zones. This is a concerning trend, but all the more so because a growing body of research, including our own preliminary study, is finding links between cognitive impairment in 9/11 responders and dementia. A recent Washington Post piece detailed how 9/11 survivors are experiencing these dementia-like conditions in their 50s – far earlier than is typical.
The COVID-19 pandemic, too, has taken a toll on those who have already suffered from 9/11. People with preexisting conditions have been at far higher risk during the pandemic. Not surprisingly, a recent study found a higher incidence of COVID-19 in WTC responders from January through August 2020.
[Get our best science, health and technology stories. Sign up for The Conversation’s science newsletter.]
Honoring the 9/11 survivors
The health risks posed by direct exposure to the acrid dust was underestimated at the time, and poorly understood. Appropriate personal protective equipment, such as P100 half-face respirators, was not available at that time.
But now, 20 years on, we know much more about the risks – and we have much greater access to protective equipment that can keep responders and recovery workers safe following disasters. Yet, too often, I see that we have not learned and applied these lessons.
For instance, in the immediate aftermath of the condominium collapse near Miami Beach in June, it took days before P100 half-face respirators were fully available and made mandatory for the responders. Other examples around the world are even worse: One year after the Beirut explosion in August 2020, very little action has been taken to investigate and manage the physical and mental health consequences among responders and the impacted community.
A similarly dire situation is occurring in the immediate aftermath of a July 2021 chemical fire in Durban, South Africa.
Applying the lessons learned from 9/11 is a critically important way to honor the victims and the brave men and women who took part in the desperate rescue and recovery efforts back on those terrible days.![]()
Roberto Lucchini, Professor of Occupational and Environmental Health Sciences, Florida International University
This article is republished from The Conversation under a Creative Commons license. Read the original article.

Many trusts say that “income” and/or “principal” are distributed for the beneficiary’s “Health, Education, Support and Maintenance,” or HEMS.
Why is the HEMS standard used, what does it mean, and how is it applied and enforced?
The HEMS standard is an “ascertainable standard”. It is an objective (measurable) standard. A non-ascertainable distribution standard — e.g., distributions for beneficiary’s comfort and happiness — is not measurable because distributions are measured by the beneficiary’s personal wishes.
Using the HEMS standard helps protect trust assets from creditors of the beneficiary, from the beneficiary’s spouse or partner, and from the beneficiary’s bad choices. The trust may allow, or require, the trustee to make distributions “for the benefit” of the beneficiary by paying such expenses directly.
The HEMS standard gives the beneficiary ascertainable and enforceable rights.
But how the HEMS standard applies depends on additional terms:
— Does the trust require HEMS distributions, i.e., the trustee “shall” make HEMS distributions — or does the trust authorize HEMS distributions at the discretion of the trustee, i.e., the trustee “may” make HEMS distributions?
— Does the trust require the trustee to consider the beneficiary’s other resources before making a HEMS distribution, i.e., the trustee “shall” first consider the beneficiary’s income and assets before making a distribution — or does the trust allow the trustee to consider the beneficiary’s other resources, i.e., the trustee “may” consider the beneficiary’s other income and assets before making a distribution?
— Does the trust give priority to some beneficiaries over other beneficiaries, e.g., the trustee shall first make distributions for the HEMS of minor children and only make HEMS distributions for adult children if there remains sufficient assets after taking into consideration the future needs of the minor children?
Saying that the trustee “may distribute” requires the trustee to exercise discretion.
In California, generally, “a discretionary power conferred upon a trustee is not left to the trustee’s arbitrary discretion, but shall be exercised reasonably (section 16080 Probate Code).
Moreover, subject to important exceptions, “if a trust instrument confers “absolute,” “sole,” or “uncontrolled” discretion on a trustee, the trustee shall act in accordance with fiduciary principles and shall not act in bad faith or in disregard of the purposes of the trust (section 16081 Probate Code).”
Next, what does “health, education, maintenance and support” include? It includes the beneficiaries “needs” — as opposed to “wants”. It is not necessarily limited to “basic needs.” The trust may define these terms, either expansively or narrowly.
Generally, “health” includes both mental and physical health. Education is often broad and may include private high school, vocational school, occupational training.
The trust may define the “education” to say whether it includes sports, room and board, computer, and a spending stipend. “Maintenance and support” means the beneficiary’s standard of living.
The trust may further define what standard of living applies. Is it limited to the “beneficiary’s accustomed manner of living” or may the trustee increase the beneficiary’s standard of living?
“Maintenance and support” includes rent, daily living expenses, transportation, utilities and vacations (amongst many others), but again may be defined.
The trustee owes a fiduciary duty to the beneficiary to faithfully and competently carry out the terms of the trust as written. The trustee must avoid conflicts of interest and may not favor one beneficiary over another (unless permitted by the trust). If the trustee breaches (violates) his or her “fiduciary duties,” the beneficiary may petition the court to require an accounting and hold the trustee accountable.
Alternatively, the beneficiary may petition the court for instructions to the trustee to order distributions.
The foregoing is a partial and simplified discussion of a larger and fact specific subject. It is not legal advice. Consult an attorney for guidance.
Dennis A. Fordham, attorney, is a State Bar-Certified Specialist in estate planning, probate and trust law. His office is at 870 S. Main St., Lakeport, Calif. He can be reached at

NASA’s Perseverance rover this week completed the collection of the first sample of Martian rock, a core from Jezero Crater slightly thicker than a pencil. Mission controllers at NASA’s Jet Propulsion Laboratory in Southern California received data that confirmed the historic milestone.
The core is now enclosed in an airtight titanium sample tube, making it available for retrieval in the future.
Through the Mars Sample Return campaign, NASA and the European Space Agency, or ESA, are planning a series of future missions to return the rover’s sample tubes to Earth for closer study. These samples would be the first set of scientifically identified and selected materials returned to our planet from another.
“NASA has a history of setting ambitious goals and then accomplishing them, reflecting our nation’s commitment to discovery and innovation,” said NASA Administrator Bill Nelson. “This is a momentous achievement and I can’t wait to see the incredible discoveries produced by Perseverance and our team.”
Along with identifying and collecting samples of rock and regolith (broken rock and dust) while searching for signs of ancient microscopic life, Perseverance’s mission includes studying the Jezero region to understand the geology and ancient habitability of the area, as well as to characterize the past climate.
“For all of NASA science, this is truly a historic moment,” said Thomas Zurbuchen, associate administrator for science at NASA Headquarters in Washington. “Just as the Apollo Moon missions demonstrated the enduring scientific value of returning samples from other worlds for analysis here on our planet, we will be doing the same with the samples Perseverance collects as part of our Mars Sample Return program. Using the most sophisticated science instruments on Earth, we expect jaw-dropping discoveries across a broad set of science areas, including exploration into the question of whether life once existed on Mars.”
First sample
The sample-taking process began on Wednesday, Sept. 1, when the rotary-percussive drill at the end of Perseverance’s robotic arm cored into a flat, briefcase-size Mars rock nicknamed “Rochette.”
After completing the coring process, the arm maneuvered the corer, bit, and sample tube so the rover’s Mastcam-Z camera instrument could image the contents of the still-unsealed tube and transmit the results back to Earth. After mission controllers confirmed the cored rock’s presence in the tube, they sent a command to complete processing of the sample.
On Monday at 12:34 a.m. EDT, Perseverance transferred sample tube serial number 266 and its Martian cargo into the rover’s interior to measure and image the rock core. It then hermetically sealed the container, took another image, and stored the tube.
“With over 3,000 parts, the Sampling and Caching System is the most complex mechanism ever sent into space,” said Larry D. James, interim director of JPL. “Our Perseverance team is excited and proud to see the system perform so well on Mars and take the first step for returning samples to Earth. We also recognize that a worldwide team of NASA, industry partners, academia, and international space agencies contributed to and share in this historic success.”
First science campaign
Perseverance is currently exploring the rocky outcrops and boulders of “Artuby,” a ridgeline of more than a half-mile bordering two geologic units believed to contain Jezero Crater’s deepest and most ancient layers of exposed bedrock.
“Getting the first sample under our belt is a huge milestone,” said Perseverance Project Scientist Ken Farley of Caltech. “When we get these samples back on Earth, they are going to tell us a great deal about some of the earliest chapters in the evolution of Mars. But however geologically intriguing the contents of sample tube 266 will be, they won’t tell the complete story of this place. There is a lot of Jezero Crater left to explore, and we will continue our journey in the months and years ahead.”
The rover’s initial science foray, which spans hundreds of sols (Martian days), will be complete when Perseverance returns to its landing site. At that point, Perseverance will have traveled between 1.6 and 3.1 miles and may have filled as many as eight of its 43 sample tubes.
After that, Perseverance will travel north, then west, toward the location of its second science campaign: Jezero Crater’s delta region. The delta is the fan-shaped remains of the spot where an ancient river met a lake within the crater. The region may be especially rich in clay minerals. On Earth, such minerals can preserve fossilized signs of ancient microscopic life and are often associated with biological processes.
More about Perseverance
A key objective for Perseverance’s mission on Mars is astrobiology, including the search for signs of ancient microbial life. The rover will characterize the planet’s geology and past climate, pave the way for human exploration of the Red Planet, and be the first mission to collect and cache Martian rock and regolith.
Subsequent NASA missions, in cooperation with ESA, would send spacecraft to Mars to collect these sealed samples from the surface and return them to Earth for in-depth analysis.
The Mars 2020 Perseverance mission is part of NASA’s Moon to Mars exploration approach, which includes Artemis missions to the Moon that will help prepare for the first human exploration mission to the Red Planet.
JPL, which is managed for NASA by Caltech in Pasadena, California, built and manages operations of the Perseverance rover.
At the end of the hour-and-a-half-long special meeting, the trustees voted to direct interim Chancellor James Houpis to develop and implement a COVID vaccine/testing requirement to increase vaccination rates for students, faculty, volunteers and staff, to be in place by the spring semester.
Six of the trustees voted for the policy, while the seventh, Jesse Ortiz, abstained.
Ortiz had sought to amend the proposed policy by requiring vaccination with no exceptions outside of the government requirements for religious and medical exemptions, but Trustee Dennise Burbank, who had offered the motion, didn’t agree to the change.
By taking the action, the Yuba Community College District joins 37 other community college districts in California that have adopted vaccine mandates for students and staff, with another district implementing a vaccination mandate just for students, district officials reported.
The other community college district that serves Lake County, the Mendocino-Lake Community College District, does not require students and employees to be vaccinated, but it is offering incentive programs.
On Aug. 12, the Yuba College trustees voted unanimously to direct the district’s leadership team to develop a vaccine and testing requirement recommendation protocol and resolution for the board's consideration in response to rising case rates across the district’s service area, which includes Lake County, as Lake County News has reported.
The cost to carry out the program is estimated at $3,465,000, including testing, student incentives, marketing, technology and staffing, including hiring four COVID tracers and a COVID manager to oversee the effort.
“This is not a vaccine mandate,” Houpis told the board during the special Thursday afternoon session.
Rather, he said it’s a requirement to either be vaccinated or have weekly testing.
Houpis also emphasized that it’s not a political issue, as people from both major political parties are encouraging vaccinations.
He said it’s disheartening that herd immunity hasn’t been achieved in 20 months, and pointed out that 35,000 people in the district’s eight county service area have been infected and more than 500 people have died during that time from an illness that is, for the most part, preventable.
With vaccination rates low for college-age individuals and college students representing a significant source of transition, and with the highly contagious Delta variant spreading, Houpis said it was incumbent on the district to move forward with a policy.
The longer it takes to move toward herd immunity, the more likely a new variant will come along that’s more contagious and deadly, Houpis said.
The plan Houpis and district leadership staff presented would require that all faculty, staff, administrators and volunteers be vaccinated effective Dec. 1, with a vaccination deadline of Jan. 24 — which also is the first day of the spring semester — for all students.
Those who don’t adhere to those deadlines must be tested weekly in order to be on district-owned or controlled premises or to participate in district activities for an extended amount of time.
Students who don’t get vaccinated also have the option of staying on distance learning.
At the same time, face coverings must be worn by everyone in all indoor settings, regardless of vaccination status.
Due to enforcement challenges, the district will require visitors to wear masks but won’t extend the vaccine or testing mandate to them. Vendors will be dealt with on a case-by-case basis.
In tracking that vaccination and testing information the policy will require the district to collect, it must follow the Confidentiality of Medical Information Act, or CMIA. The Health Insurance Portability and Accountability Act, or HIPAA, does not generally apply to schools.
Based on the timelines for implementing the program, the district’s new vaccination tracking system prototype must be in testing by Oct. 15, with that testing to be complete by Oct. 29 and in production from Nov. 12 to 14, as registration for the fall semester starts Nov. 15. The contact tracing system must be in production by Sept. 30, and ready to integrate with vaccine records by Jan. 24.
Ortiz said testing is not an alternative to vaccination, pointing to more than 600,000 Americans who have died from COVID-19.
He said people of color are disproportionately affected by the virus, adding that 70% of the district’s students are people of color. “Either we're in this all the way or we're not.”
Trustee David Wheeler also suggested a very strong policy with exceptions only for medical reasons.
Jake Hurley, associate vice chancellor of human resources, said the Equal Employment Opportunity Commission allows the district to mandate vaccinations for staff, but they must offer medical and religious exemptions, which the policy presented to the board does.
However, Hurley noted that people who don’t want to get vaccinated will exploit those loopholes. “That’s the reality.”
Ultimately, the board agreed to go with the policy staff presented, requiring vaccination or testing.
A concern voiced during the meeting was whether or not the district’s enrollment, which has been in decline, could see further drops because of the policy.
However, it also was suggested that the policy may increase enrollment as students — eager to get back to face-to-face instruction — feel safer being back on campus.
Email Elizabeth Larson at

LAKE COUNTY, Calif. — Officials reported that recent testing of sites on Clear Lake have shown dangerous levels of cyanotoxin.
While much of the aquatic plant growth visible in the lake right now is harmless, cyanobacteria, when present in sufficient abundance, can produce cyanotoxins, which pose health hazards to humans, livestock and pets.
Water monitoring is regularly conducted by the Big Valley Band of Pomo Indians with assistance from Robinson Rancheria EPA Department, at approximately 15 Clear Lake sites.
All verified results are publicly available here.
Currently, concentrations of microcystin cyanotoxin at numerous locations around the lake are extremely high.
During recent sampling conducted on Tuesday, Aug. 25, EPA lab-confirmed testing indicated the highest levels of two toxins that have been recorded on Clear Lake during water sampling events: a microcystin (liver toxin) result value of almost 26,000 micrograms per liter (µg/L) and an anatoxin-a (neurotoxin) result value of almost 13 µg/L.
The nine locations with DANGER levels of Cyanotoxin are the following (also see yellow CAUTION indicators on the map, below):
— Clearlake Oaks (CLOAKS01, Oaks Arm).
— Elem Indian Colony shoreline (ELEM01, Oaks Arm).
— Sulphur Bank Mercury Mine shoreline (SBMMEL01, Oaks Arm).
— Lily Cove (LC01, Lower Arm).
— Austin Park (AP01, Lower Arm).
— Redbud Park (RED01, Lower Arm).
— Shady Acres (SHADY01, Cache Creek).
— Jago Bay (JB, Lower Arm).
— Lakeport, Library Park (LPTNT, Upper Arm).
Public Health urges boaters and other recreational lake users to avoid direct contact with or use of waters containing cyanobacteria in Lake County and to follow all posted signage regarding safe activities.
This recommendation is based on the recent toxin results as well as the potential health risks from cyanobacteria, which is currently blooming at varying levels throughout the lake.
Cyanobacteria can pose health risks, particularly to children and pets. Officials urge people to choose safe activities when visiting natural bodies of water, particularly where blooms are visible.
It is strongly recommended people and their pets avoid contact with and avoid swallowing lake water in areas where algal blooms are present.
Conditions can quickly change. Before recreating in Clear Lake, check the most recent monitoring results.
For current cyanotoxin lab results, please visit the Big Valley Band of Pomo Indians cyanotoxin monitoring website and Clear Lake Water Quality Facebook page.
Further resources are available at the following webpages:
http://www.lakecountyca.gov/cyanobacteria/
http://www.lakecountyca.gov/cyanohealth/
California Portal on Harmful Algal Blooms:
https://mywaterquality.ca.gov/habs/index.html
CDC guidance regarding harmful algal blooms can be found here:
https://www.cdc.gov/habs/materials/factsheet-cyanobacterial-habs.html

The World Health Organization, or WHO, declared COVID-19 a pandemic on March 11, 2020.
After that, many doctors in the U.S. delayed elective medical procedures and Medical and Diagnostic Laboratories developed a variety of COVID-19 tests.
Did those changes have uneven economic impacts on health care operations?
They did, according to an analysis of the Census Bureau’s Quarterly Services Survey, or QSS, data on doctor visits, lab and diagnostic testing, and hospital visits.
The data show that some health care industries that normally follow similar economic patterns diverged in some quarters during the pandemic.
All revenue data contained in this article are seasonally adjusted, but hospital inpatient days and discharges data are not.
The data show that some health care industries that normally follow similar economic patterns diverged in some quarters during the pandemic.
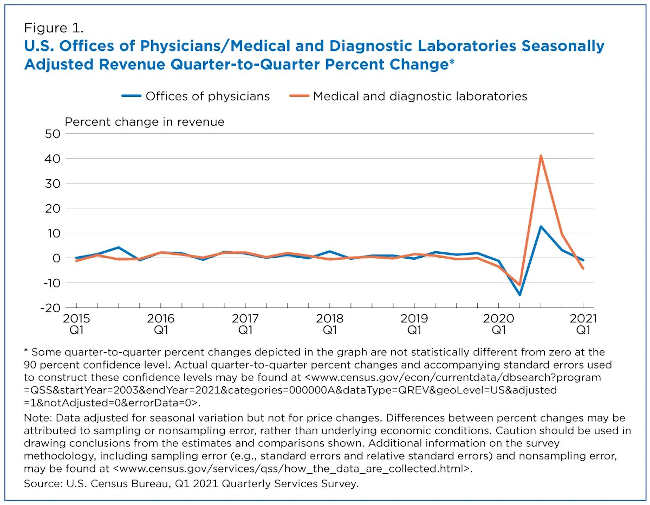
For example, before the pandemic, visiting the doctor and getting lab tests were commonly linked (Figure 1). But during the pandemic, lab testing surged higher than visits to doctors’ offices — a shift known as divergence.
While the revenue of both Offices of Physicians and Medical and Diagnostic Laboratories fell significantly in the second quarter of 2020 — down 14.9% and 10.9% respectively from the first quarter of 2020 — there was some divergence afterward.
In the third quarter of 2020, revenue for Medical and Diagnostic Laboratories increased 41.1% from the previous quarter. Nationwide COVID-19 testing was a central factor.
Revenue for the Offices of Physicians also rebounded in the third quarter of 2020, but the 12.6% quarter-to-quarter change was not as pronounced as the increase for Medical and Diagnostic Laboratories.
A tale of two recoveries
By the fourth quarter of 2020 and first quarter of 2021, the percentage changes had decreased compared to the spikes in the third quarter of 2020 for both industries.
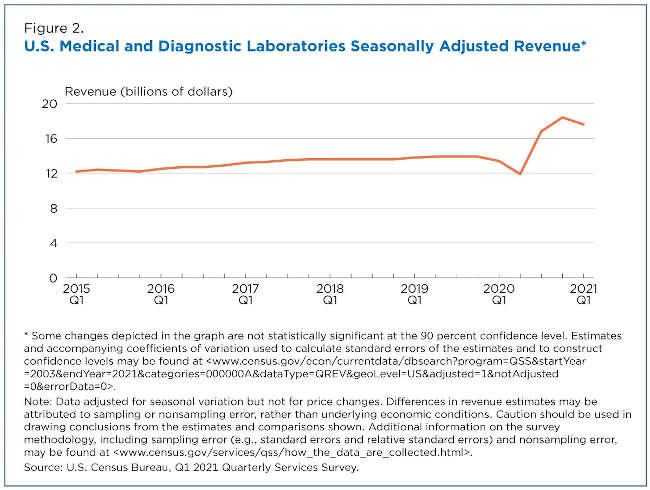
However, it’s notable that revenue of Medical and Diagnostic Laboratories remained much higher than before COVID-19 (Figure 2).
Total revenue of Medical and Diagnostic Laboratories increased 9.4% from $16.8 billion in the third quarter to $18.4 billion in the fourth quarter of 2020. But it fell 4.3% to $17.6 billion in the first quarter of 2021.
Importantly, total revenue in the first quarter of 2021 was higher than the $13.4 billion in the first quarter of 2020.
The QSS estimates show that total revenue levels for Medical and Diagnostic Laboratories remain elevated during widespread COVID-19 testing in the United States. In fact, the Centers for Disease Control (CDC) Data Tracker tallied more than 375 million COVID-19 RT-PCR tests by the end of the first quarter of 2021.
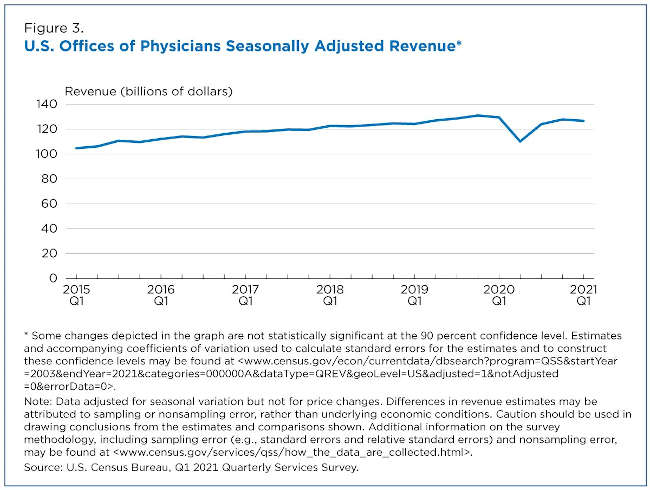
In contrast, total revenue for Offices of Physicians was approximately $129.5 billion in the first quarter of 2020 and $126.7 billion in the first quarter of 2021 — a year-over-year change that is not significant (Figure 3).
This implies that the volume of routine office visits in the first quarter of 2021 weren’t much different from when the pandemic began in the first quarter of 2020. One February 2021 study by The Harris Poll found that 27% of 1,093 U.S. adults polled had delayed annual checkups in the prior three months.
Hospital services and tax breakouts
The Coronavirus Aid, Relief, and Economic Security, or CARES, Act was signed into law March 27, 2020, in response to the economic uncertainties created by the COVID-19 pandemic.
Subsequently, the U.S. Department of Health and Human Services, or HHS, established the Provider Relief Fund program. Relief funds were distributed to the nation’s Hospitals, tax-exempt and taxable alike.
It is important to note that the QSS collects revenue differently between tax-exempt and taxable firms on its hospital survey forms.
The QSS asks tax-exempt firms to include nonoperating grant revenue in the calculation of total revenue as it’s generally a routine source of revenue for tax-exempt hospitals. However, the QSS asks taxable firms to exclude nonoperating grant revenue in the calculation of total revenue as it’s generally not a routine source of revenue for taxable hospitals.
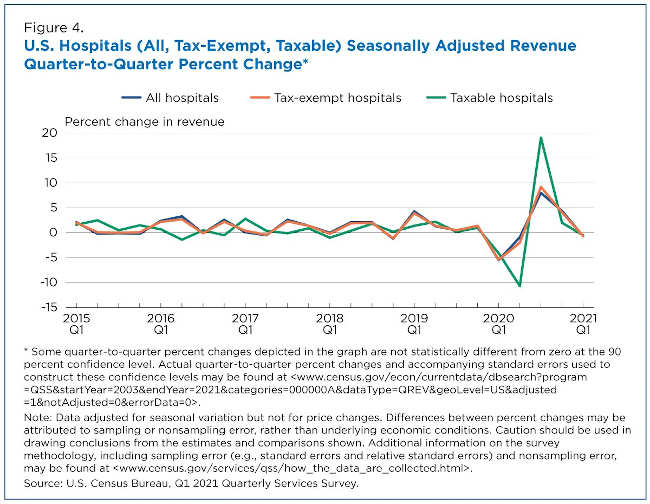
The quarter-to-quarter percentage changes for the hospital industry closely mirror its largest subset: tax-exempt hospitals that make up approximately 88% of the industry (Figure 4).
The QSS data show that revenue for tax-exempt hospitals dropped 5.5% in the first quarter of 2020. Revenue for taxable hospitals dropped 4.1% in the first quarter and another 10.7% in the second quarter of 2020.
Hospital revenue increased significantly in the third quarter of 2020 with taxable hospitals up the most with a 19.1% increase from the second quarter of 2020. By the first quarter of 2021, total revenue for the hospital industry was up 10.6% compared to the first quarter of 2020.
Hospital inpatient days and discharges
Based on the revenue growth, one might think that year-over-year percentage increases in revenue would mean more volume for America’s hospitals. The QSS data tell a different story.
For QSS, inpatient days measure the length of a hospital stay during which services were provided to inpatients. A discharge is the formal release of the patient (including those admitted and discharged on the same day).
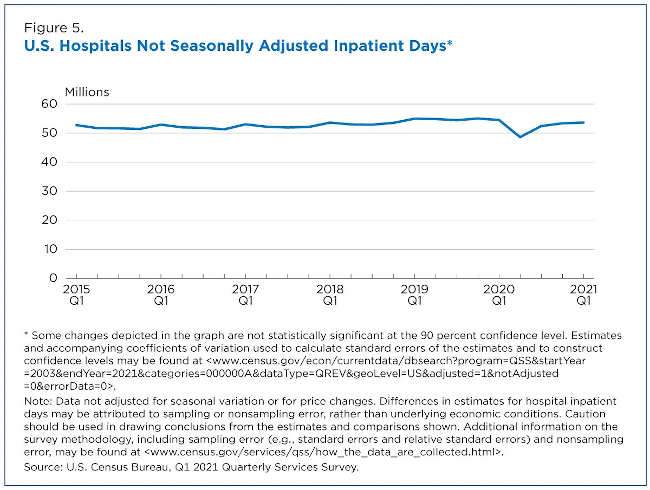
Hospital inpatient days dropped from approximately 54.5 million in the first quarter of 2020 to 48.6 million in the second quarter of 2020 — a decrease of 10.8%. The decline could be due to fewer elective surgeries being scheduled during the early part of the pandemic as recommended by the Centers for Medicare & Medicaid Services (CMS).
By the first quarter of 2021, inpatient days were 53.6 million (Figure 5).
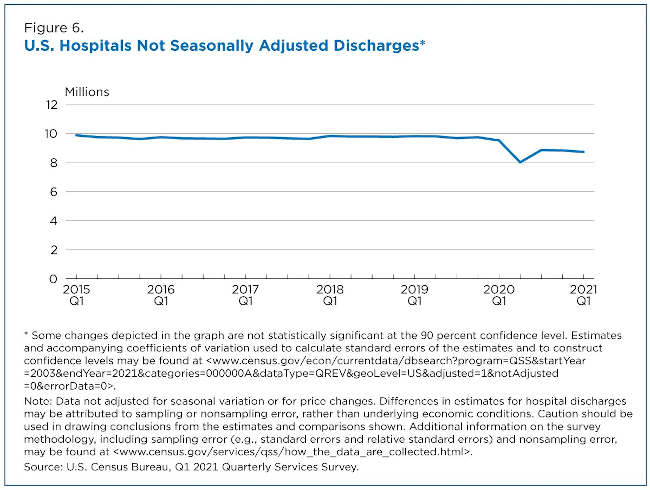
Hospital discharges dropped 15.9% from approximately 9.5 million in the first quarter of 2020 to 8.0 million in the second quarter of 2020. By the first quarter of 2021, there were 8.7 million discharges (Figure 6).
QSS data indicate that hospital revenue percentage change was up in the first quarter of 2021 from the first quarter of 2020. However, hospital inpatient days and discharges show that volume wasn’t significantly different year-over-year.
Some private sector reports support this result as hospital volume metrics, particularly emergency room visits, continued to lag.
The health care industries above demonstrate how the COVID-19 pandemic has unevenly affected a key sector in the U.S. economy — a sector facing one of its greatest public health challenges in decades.
Justin Jarrett is a survey statistician in the Census Bureau’s Economic Indicators Division.